Explain How Climate and Temperature Can Affect the Behavior of Individuals.
Climate Change and Homo Health
Introduction
- John Balbus
National Institutes of Health - Allison R. Crimmins
U.Southward. Environmental Protection Agency - Janet 50. Chance
U.S. Ecology Protection Agency
- David R. Easterling
National Oceanic and Atmospheric Assistants - Kenneth Eastward. Kunkel
Cooperative Institute for Climate and Satellites - NC - Shubhayu Saha
Centers for Illness Control and Prevention - Marcus C. Sarofim
U.S. Environmental Protection Bureau
Human
Given that the impacts of climatic change are projected to increase over the adjacent century, certain existing health threats will intensify and new health threats may emerge. Connecting our understanding of how climate is changing with an understanding of how those changes may bear on homo health tin can inform decisions about mitigating (reducing) the corporeality of future climate change, suggest priorities for protecting public health, and aid place research needs.
1.i Our Irresolute Climate
Observed Climatic change
The fact that the Earth has warmed over the last century is unequivocal. Multiple observations of air and ocean temperatures, sea level, and snow and ice have shown these changes to be unprecedented over decades to millennia. Man influence has been the dominant cause of this observed warming.i The 2022 U.S. National Climate Assessment (2014
The concepts of climate and weather are often confused. Atmospheric conditionis the state of the atmosphere at any given time and place. Weather patterns vary greatly from year to year and from region to region. Familiar aspects of weather include temperature, precipitation, clouds, and air current that people experience throughout the course of a 24-hour interval. Severe weather weather include hurricanes, tornadoes, blizzards, and droughts. Climateis the average weather conditions that persist over multiple decades or longer. While the atmospheric condition can change in minutes or hours, identifying a change in climate has required observations over a time menses of decades to centuries or longer. Climate change encompasses both increases and decreases in temperature as well as shifts in precipitation, irresolute risks of certain types of astringent weather events, and changes to other features of the climate organization.
Effigy ane.1: Major U.Due south. Climate Trends
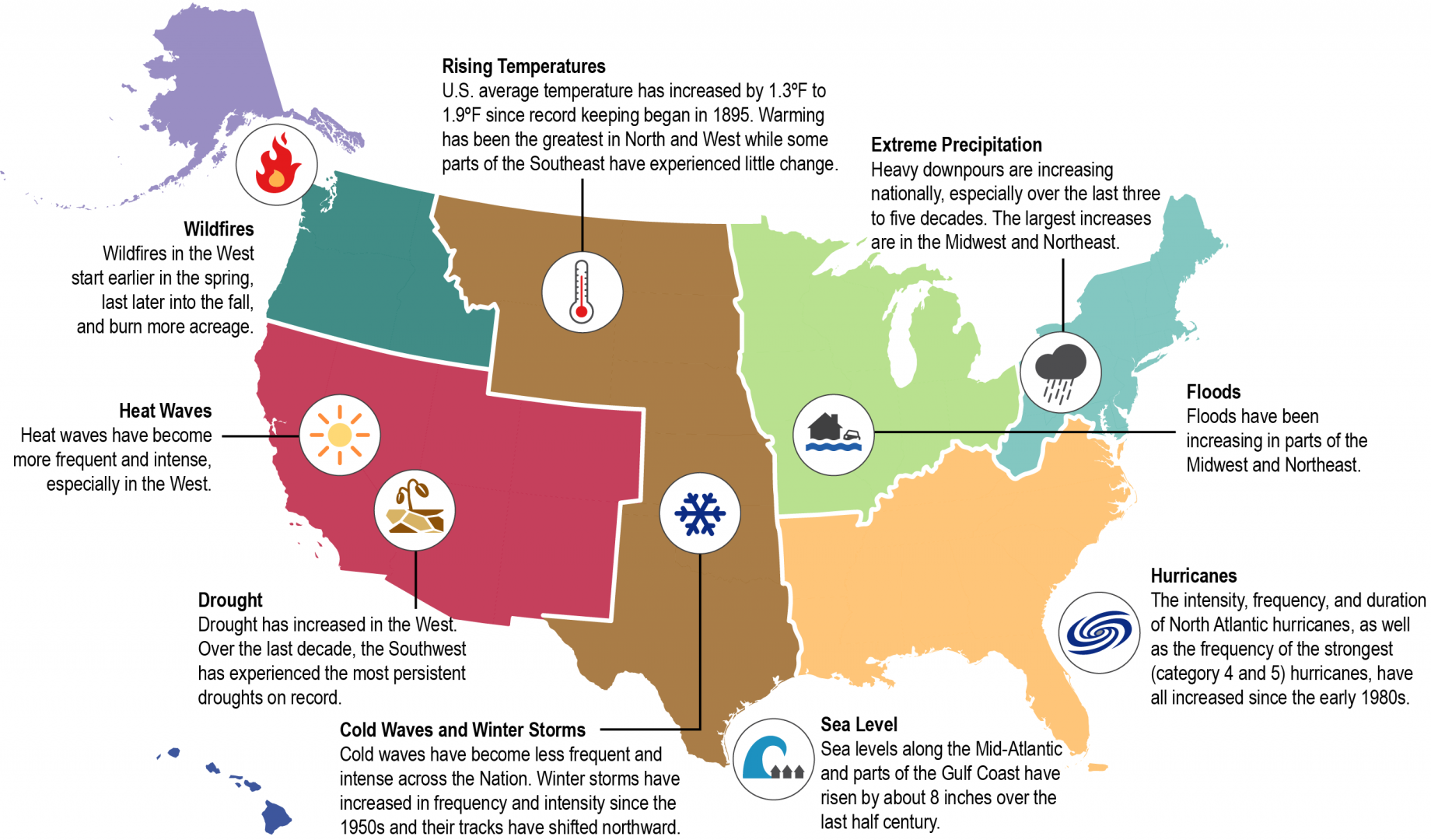
Major U.Southward. national and regional
trends. Shaded areas are the U.Southward. regions defined in the 2014
.two , 4
Observed changes in climate and weather differ at local and regional scales (Figure ane.1). Some climate and weather changes already observed in the United States include:2 , iii
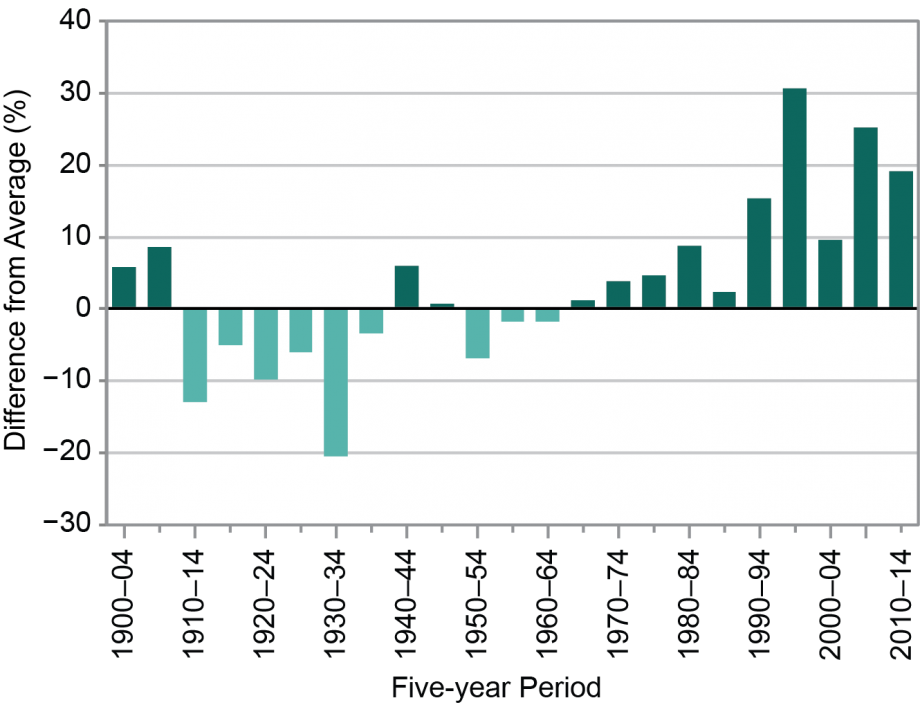
Effigy 1.2: Change in Number of Extreme Precipitation Events
VIEW
Fourth dimension series of 5-year averages of the number of extreme ii-solar day duration precipitation events, averaged over the United states of america from 1900 to 2014. The number is expressed as the percent difference from the average for the entire period. This is based on 726 stations that have precipitation data for at to the lowest degree 90% of the days in the period. An result is considered extreme if the precipitation amount exceeds a threshold for a once-per-twelvemonth recurrence. (Figure source: adapted from Mellilo et al. 2014)2
- U.Southward. average temperature has increased by i.3°F to 1.ix°F since recordkeeping began in 1895; well-nigh of this increase has occurred since about 1970. The first decade of the 2000s (2000–2009) was the warmest on record throughout the United States.
- Average U.S. precipitation has increased since 1900, but some areas accept experienced increases greater than the national average, and some areas have experienced decreases.
- Heavy downpours are increasing nationally, especially over the last three to 5 decades. The largest increases are in the Midwest and Northeast, where floods have also been increasing. Effigy 1.2 shows how the annual number of heavy downpours, defined as farthermost 2-day precipitation events, for the face-to-face Usa has increased, particularly between the 1950s and the 2000s.
-
Drought has increased in the West. Over the last decade, the Southwest has experienced the most persistent droughts since tape keeping began in 1895.four Changes in atmospheric precipitation and runoff, combined with changes in consumption and withdrawal, have reduced surface and groundwater supplies in many areas. - At that place take been changes in some other types of extreme weather events over the last several decades. Rut waves have get more frequent and intense, specially in the West. Common cold waves have become less frequent and intense beyond the nation.
- The intensity, frequency, and duration of North Atlantic hurricanes, as well as the frequency of the strongest (category 4 and 5) hurricanes, have all increased since the early on 1980s. The relative contributions of human and natural causes to these increases remain uncertain.
Projected Climate change
Projections of future climate atmospheric condition are based on results from climate models—sophisticated computer programs that simulate the behavior of the Earth'southward climate system. These climate models are used to project how the climate system is expected to change under different possible scenarios. These scenarios depict future changes in atmospheric greenhouse gas concentrations,
Figure 1.3: Projected Changes in Temperature and Precipitation by Mid-Century
Collaborate with the Figure Below
Projected changes in annual average temperature (left) and precipitation (right) for 2021–2050 and 2041–2070 with respect to the boilerplate for 1971–2000 for the RCP6.0
. The RCP6.0 pathway projects an average global temperature increase of five.2°F in 2100 over the 1901–1960 global average temperature (the RCPs are described in more particular in Appendix 1: Technical Support Document). Temperature increases in the The states for this scenario are in the 2°F to 3°F range for 2022 to 2050 and 2°F to 4°F for 2041 to 2070. This means that the increase in temperature projected in the Usa over the next 50 years under this scenario would exist larger than the i°F to 2°F increase in temperature that has already been observed over the previous century. Precipitation is projected to decrease in the Southwest and increase in the Northeast. These projected changes are statistically significant (95% confidence) in pocket-size portions of the Northeast, equally indicated past the hatching. (Figure source: adapted from Lord's day et al. 2015) 7
Some of the projected changes in climate in the Us every bit described in the 2022 NCA are listed below:2 , 3
- Temperatures in the United States are expected to continue to rising. This temperature rise has not been, and volition not exist, compatible across the country or over time (Figure one.iii).
- Increases are also projected for extreme temperature conditions. The temperature of both the hottest day and coldest night of the year are projected to increase (Effigy 1.4).
- More winter and jump precipitation is projected for the northern Usa, and less for the Southwest, over this century (Effigy one.3).
- Increases in the frequency and intensity of extreme precipitation events are projected for all U.S. areas (Figure ane.4).
- Short-term (seasonal or shorter) droughts are expected to intensify in virtually U.Due south. regions. Longer-term droughts are expected to intensify in large areas of the Southwest, the southern Cracking Plains, and the Southeast. Trends in reduced surface and groundwater supplies in many areas are expected to continue, increasing the likelihood of water shortages for many uses.
- Heat waves are projected to become more than intense, and cold waves less intense, everywhere in the Usa.
- Hurricane-associated storm intensity and rainfall rates are projected to increment as the climate continues to warm.
Figure i.four: Projected Changes in the Hottest/Coldest and Wettest/Driest Solar day of the Year
Interact with the Figure Below
Projected changes in several
variables for 2046–2065 with respect to the 1981–2000 average for the RCP6.0
. These include the coldest night of the twelvemonth and the hottest day of the twelvemonth. Past the middle of this century, the coldest night of the yr is projected to warm past six°F to ten°F over most of the state, with slightly smaller changes in the south. The warmest mean solar day of the year is projected to be iv°F to 6°F warmer in well-nigh areas. Likewise shown in a higher place are projections of the wettest day of the year and the annual longest sequent dry out day spell. Farthermost precipitation is projected to increment, with an average alter of 5% to fifteen% in the precipitation falling on the wettest mean solar day of the year. The length of the annual longest dry spell is projected to increase in almost areas, merely these changes are small: less than two days in most areas. (Figure source: adapted from Sun et al. 2015)7
1.2 How Does Climatic change Affect Wellness?
The influences of
A useful approach to understand how climatic change affects wellness is to consider specific
Whether or not a person is exposed to a health threat or suffers disease or other adverse health outcomes from that exposure depends on a complex ready of
- Exposure is contact between a person and one or more biological, psychosocial, chemical, or physical stressors, including stressors affected by climate change. Contact may occur in a unmarried case or repeatedly over time, and may occur in one location or over a wider geographic expanse.
- Sensitivity is the degree to which people or communities are affected, either adversely or beneficially, past
climate variability or alter. -
Adaptive chapters is the ability of communities, institutions, or people to adjust to potential hazards, to take advantage of opportunities, or to respond to consequences. A related term, resilience, is the ability to prepare and plan for, absorb, recover from, and more successfully arrange to agin events.
(definitions adjusted from
Vulnerability, and the three components of vulnerability, are factors that operate at multiple levels, from the individual and community to the country level, and affect all people to some caste.9 For an individual, these factors include homo behavioral choices and the degree to which that person is vulnerable based on his or her level of exposure, sensitivity, and adaptive capacity. Vulnerability is also influenced by
At a larger customs or societal scale, health outcomes are strongly influenced by adaptive capacity factors, including those related to the natural and congenital environments (for example, the country of
The iii components of vulnerability (exposure, sensitivity, and adaptive capacity) are associated with social and
Figure i.5: Climate Change and Health
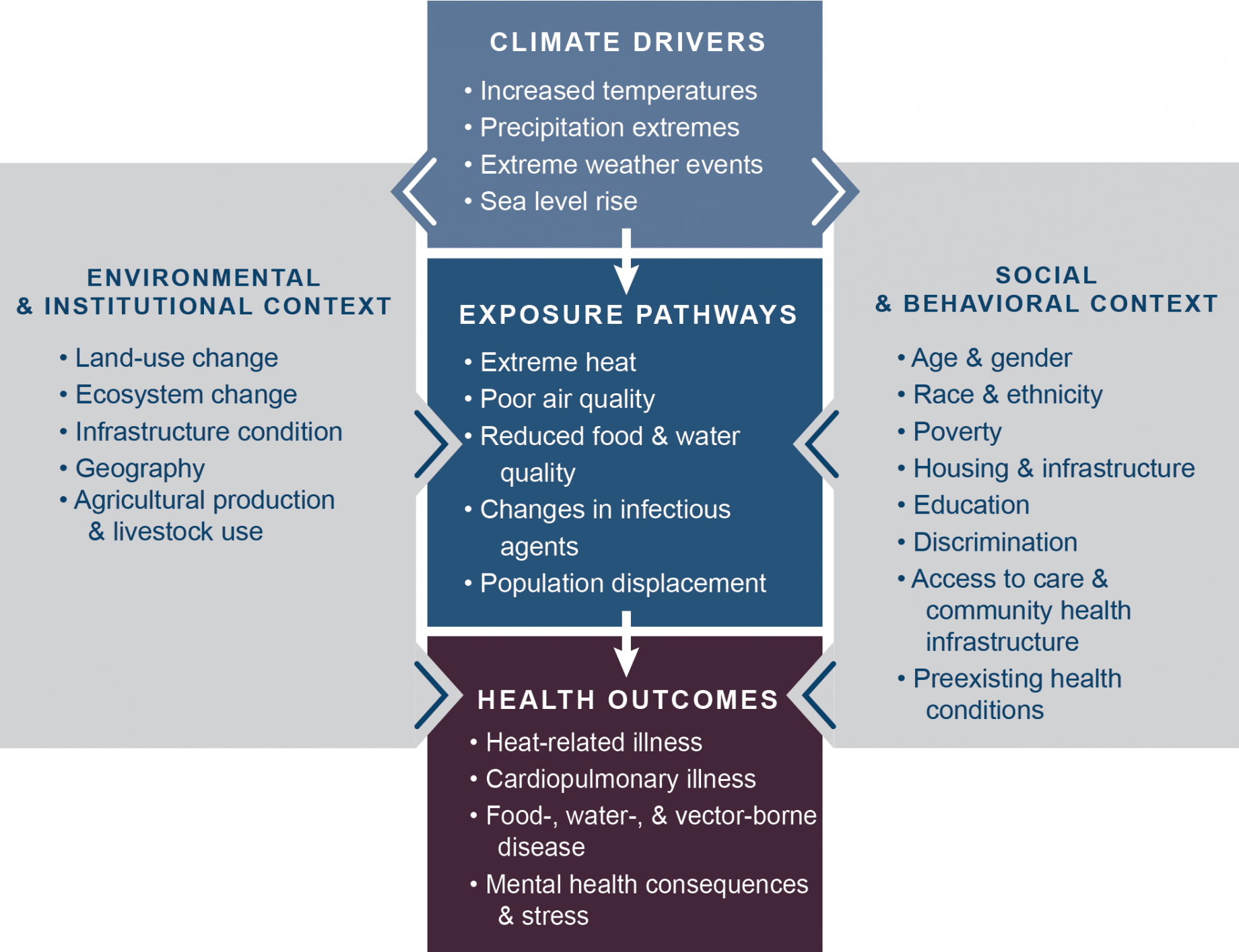
Conceptual diagram illustrating the
pathways by which
affects human
. Exposure pathways exist inside the context of other factors that positively or negatively influence wellness outcomes (gray side boxes). Key factors that influence
for individuals are shown in the right box, and include
and behavioral choices. Key factors that influence vulnerability at larger scales, such as natural and built environments, governance and management, and institutions, are shown in the left box. All of these influencing factors tin bear upon an private's or a customs'southward vulnerability through changes in exposure,
, and
and may also be affected by climate alter.
We are already experiencing changes in the frequency, severity, and even the location of some conditions and climate phenomena, including farthermost temperatures, heavy rains and droughts, and some other kinds of severe weather, and these changes are projected to continue. This means that areas already experiencing health-threatening weather and climate phenomena, such as severe oestrus or hurricanes, are likely to experience worsening impacts, such as even higher temperatures and increased storm intensity, rainfall rates, and
Climatic change can therefore affect human health in two principal ways: first, by changing the severity or frequency of health problems that are already afflicted by climate or atmospheric condition factors; and 2d, past creating unprecedented or unanticipated health problems or health threats in places where they have not previously occurred.
1.three Our Irresolute Health
In order to empathise how
Demographic and Socioeconomic Trends
The Usa is in the midst of several pregnant demographic changes: the population is aging, growing in number, becoming more ethnically diverse, and demonstrating greater disparities between the wealthy and the poor. Immigration is having a major influence on both the size and age distribution of the population.15 Each of these demographic trends has implications for climatic change related human wellness impacts (meet Ch. nine: Populations of Concern). Some of these trends and projections are summarized below:
Trends in population growth
- The total U.South. population has more than than doubled since 1950, from 151,325,798 persons in 1950 to 308,745,538 in 2010.16
- The Census Bureau projects that the U.S. population will abound to almost 400 million by 2050 (from estimates of well-nigh 320 meg in 2014).17
Trends in the elderly population
- The nation'due south older adult population (ages 65 and older) will most double in number from 2022 through 2050, from approximately 48 one thousand thousand to 88 one thousand thousand.18 Of those 88 1000000 older adults, a little under xix million volition be 85 years of historic period and older.19
Trends in racial and indigenous diversity
- As the U.s.a. becomes more diverse, the amass minority population is projected to become the majority by 2042.18 The non-Hispanic or not-Latino White population volition increase, but more slowly than other racial groups. Not-Hispanic Whites are projected to become a minority by 2050.20
- Projections for 2050 suggest that nearly 19% of the population will be immigrants, compared with 12% in 2005.twenty
- The Hispanic population is projected to nearly double from 12.5% of the U.S. population in 2000 to 24.six% in 2050.21
Trends in economic disparity
- Income inequality rose and then stabilized during the concluding xxx years, and is projected to resume rising over the next twenty years, though at a somewhat slower overall rate that declines to near zero by 2035.22 For example, the Gini coefficient, a measure out of income inequality, is estimated to have risen past xviii% betwixt 1984 and 2000, and is projected to rise by an additional 17% for all workers between 2009 and 2035.22
- America's communities of color have disproportionately higher poverty rates and lower income levels. While racial disparities in household wealth were college in the late 1980s than now, trends in more contempo years take been toward greater inequality. The ratio of the median net household worth of White, not-Hispanic versus non-White or Hispanic households increased from 6.0 to 7.eight between 2007 and 2013.23 In 2009, 25.8% of non-Hispanic Blacks and 25.3% of Hispanics had incomes beneath the poverty level as compared to nine.iv% of non-Hispanic Whites and 12.five% of Asian Americans.24 In 2014, the median income level for a not-Hispanic Blackness household was approximately $35,000, $25,000 lower than a non-Hispanic White household.25
Population growth and migration in the Usa may place more than people at
Trends in Health Condition

Tempest-damaged home after Hurricane Sandy © iStockPhoto. com/Aneese
Every bit a nation, trends in the population'southward health are mixed. Some major indicators of health, such as life expectancy, are consistently improving, while others, such as rate and number of
Climate modify impacts to human health volition act on top of these underlying trends. Some of these underlying health conditions can increase
Examples of health indicators that have been improving between 2000 and 2022 include the following:
- Life expectancy at nativity increased from 76.eight to 78.8 years.thirty
- Decease rates per 100,000 people from heart illness and cancer decreased from 257.six to 169.viii and from 199.half-dozen to 163.2, respectively.30
- The percentage of people over age eighteen who say they smoke decreased from 23.2% to 17.8%.30

© Monkey Concern Images/Corbis
At the same time, some health trends related to the prevalence of
- The percentage of adult (18 years and older) Americans describing their health as "poor or fair" increased from 8.9% in 2000 to 10.3% in 2012.xxx
- Prevalence of physician-diagnosed diabetes amid adults anile 20 and over increased from 5.ii% in 1988-1994 to viii.4% in 2009-2012.30
- The prevalence of obesity among adults (anile twenty–74) increased past almost three-fold from 1960–1962 (xiii.iv% of adults classified as obese) to 2009–2010 (36.one% of adults classified as obese).31
- In the past thirty years, obesity has more doubled in children and quadrupled in adolescents in the Usa. The percentage of children aged half-dozen–11 who were obese increased from 7% in 1980 to nearly eighteen% in 2012. Similarly, the per centum of adolescents aged 12–nineteen years who were obese increased from 5% to well-nigh 21% over the same period. In 2012, approximately one-3rd of American children and adolescents were overweight or obese.32
Tabular array 1.1 shows some examples of underlying health conditions that are associated with increased vulnerability to health effects from climate change related exposures (come across Ch. 9: Populations of Concern for more details) and provides information on current status and future trends.
Wellness condition is often associated with demographics and socioeconomic status. Changes in the overall size of the population, racial and ethnic composition, and historic period distribution impact the health condition of the population. Poverty, educational attainment, access to care, and discrimination all contribute to disparities in the incidence and prevalence of a variety of medical weather condition (run into Ch. 9: Populations of Concern). Some examples of these interactions include:
Older Adults. In 2013, the percentage of adults age 75 and older described as persons in fair or poor health totaled 27.6%, as compared to 6.2% for adults age 18 to 44.30Amongst adults age 65 and older, the number in nursing homes or other residential care facilities totaled one.8 million in 2012, with more than 1 million utilizing home wellness care.33
© Stephen Welstead/LWA/ Corbis
Children. Approximately 9.0% of children in the United States have asthma. Betwixt 2022 and 2013, rates for Blackness (xv.3%) and Hispanic (8.6%) children were higher than the rate for White (7.8%) children.30 Rates of asthma were also higher in poor children who alive below 100% of the poverty level (12.iv%).30
Non-Hispanic Blacks. In 2014, the percentage of non-Hispanic Blacks of all ages who were described as persons in fair or poor health totaled 14.3% equally compared to 8.7% for Whites. Wellness risk factors for this population include high rates of smoking, obesity, and
Hispanics. The percentage of Hispanics of all ages who were described as persons in off-white or poor health totaled 12.7% in 2014. Wellness disparities for Hispanics include moderately higher rates of smoking in adults, depression birth weights, and infant deaths.thirty
The impacts of climatic change may worsen these health disparities by exacerbating some of the underlying atmospheric condition they create. For example, disparities in life expectancy may be exacerbated by the effects of climate change related estrus and air pollution on minority populations that have higher rates of hypertension, smoking, and diabetes. Conversely, public health measures that reduce disparities and overall rates of illness in populations would lessen vulnerability to worsening of health status from climate alter furnishings.
Table 1.1: Current estimates and future trends in chronic health conditions that interact with the wellness risks associated with climate change
Click on a table row for more information.
| | Electric current Estimates | Future Trends | Possible Influences of |
|---|---|---|---|
| ALZHEIMER'S Affliction | Approximately 5 million Americans over 65 had Alzheimer'southward disease in 2013.34 | | Persons with |
| | Average asthma prevalence in the U.South. was higher in children (9% in 2014)30 than in adults (vii% in 2013).35 Since the 1980s, asthma prevalence increased, but rates of asthma deaths and hospital admissions declined.36 , 37 | Stable | Asthma is exacerbated past changes in pollen flavor and allergenicity and in exposures to air pollutants afflicted past changes in temperature, humidity, and wind.29 |
| | In 2012, approximately half-dozen.three% of adults had COPD. Deaths from chronic lung diseases increased past 50% from 1980 to 2010.38 , 39 | Chronic | COPD patients are more sensitive than the general population to changes in ambience air quality associated with climate modify. |
| | In 2012, approximately 9% of the full U.South. population had diabetes. Approximately 18,400 people younger than age 20 were newly diagnosed with type 1 diabetes in 2008–2009; an additional 5,000 were diagnosed with blazon ii. forty | New diabetes cases are projected to increase from almost 8 cases per 1,000 in 2008 to almost 15 per one,000 in 2050. If recent increases proceed, prevalence is projected to increase to 33% of Americans by 2050. 41 | Diabetes increases |
| | Cardiovascular disease ( | By 2030, approximately 41% of the U.Southward. population is projected to accept some form of CVD.43 | Cardiovascular disease increases sensitivity to rut stress. |
| MENTAL Affliction | | By 2050, the full number of U.South. adults with depressive disorder is projected to increase by 35%, from 33.9 1000000 to 45.8 million, with those over age 65 having a 117% increase. 44 | Mental illness may impair responses to |
| | In 2009–2010, approximately 35% of American adults were obese.32 In 2012, approximately 32% of youth (anile ii–19) were overweight or obese.46 , 47 | Past 2030, 51% of the U.S. population is expected to exist obese. Projections suggest a 33% increase in obesity and a 130% increase in astringent obesity.48 | Obesity increases sensitivity to high ambience temperatures. |
| | Approximately 18.7% of the U.S. population has a inability. In 2010, the per centum of American adults with a disability was approximately 16.6% for those age 21–64 and 49.8% for persons 65 and older. 49 | The number of older adults with activity limitations is expected to grow from 22 one thousand thousand in 2005 to 38 million in 2030.l | Persons with disabilities may find it difficult to respond when evacuation is required and when there is no bachelor means of transportation or easy exit from residences. |
1.four Quantifying Wellness Impacts
For some changes in exposures to

The ability to quantify many types of wellness impacts is dependent on the availability of data on the baseline
Information on trends in underlying health or background rates of health impacts is summarized in Section 1.3, "Our Changing Health." Data on the incidence and prevalence of health conditions are obtained through a complicated system of state- and city-level
Characterizing certain types of climatic change related exposures can be a challenge. Exposures can consist of temperature changes and other
Modeling Approaches Used in this Report
Four chapters inside this assessment—Ch. two: Temperature-Related Death and Illness, Ch. iii: Air Quality Impacts, Ch. 5: Vector-Borne Diseases, and Ch. half dozen: Water-Related Illness—include new peer-reviewed, quantitative analyses based on modeling. The analyses highlighted in these chapters mainly relied on climate model output from the Coupled Model Intercomparison Projection Phase 5 (CMIP5). Due to limited data availability and computational resources, the studies highlighted in the iv capacity analyzed only a subset of the full CMIP5 dataset, with most of the studies including at least one analysis based on RCP6.0, an upper midrange greenhouse gas concentration pathway, to facilitate comparisons across capacity. For example, the air quality analysis examined results from 2 unlike RCPs, with a dissimilar climate model used for each, while the waterborne analyses examined results from 21 of the CMIP5 models for a single
Adverse wellness effects attributed to climatic change tin can have many economic and social consequences, including directly medical costs, work loss, increased care giving, and other limitations on everyday activities. Though economic impacts are a crucial component to agreement risk from climate change, and may have important directly and secondary impacts on homo health and well-being by reducing resources available for other preventative health measures, economic valuation of the health impacts was not reported in this assessment.
Uncertainty in Health Bear upon Assessments
Figure 1.6 illustrates dissimilar sources of uncertainty along the exposure pathway.
Figure i.half dozen: Sources of Doubtfulness
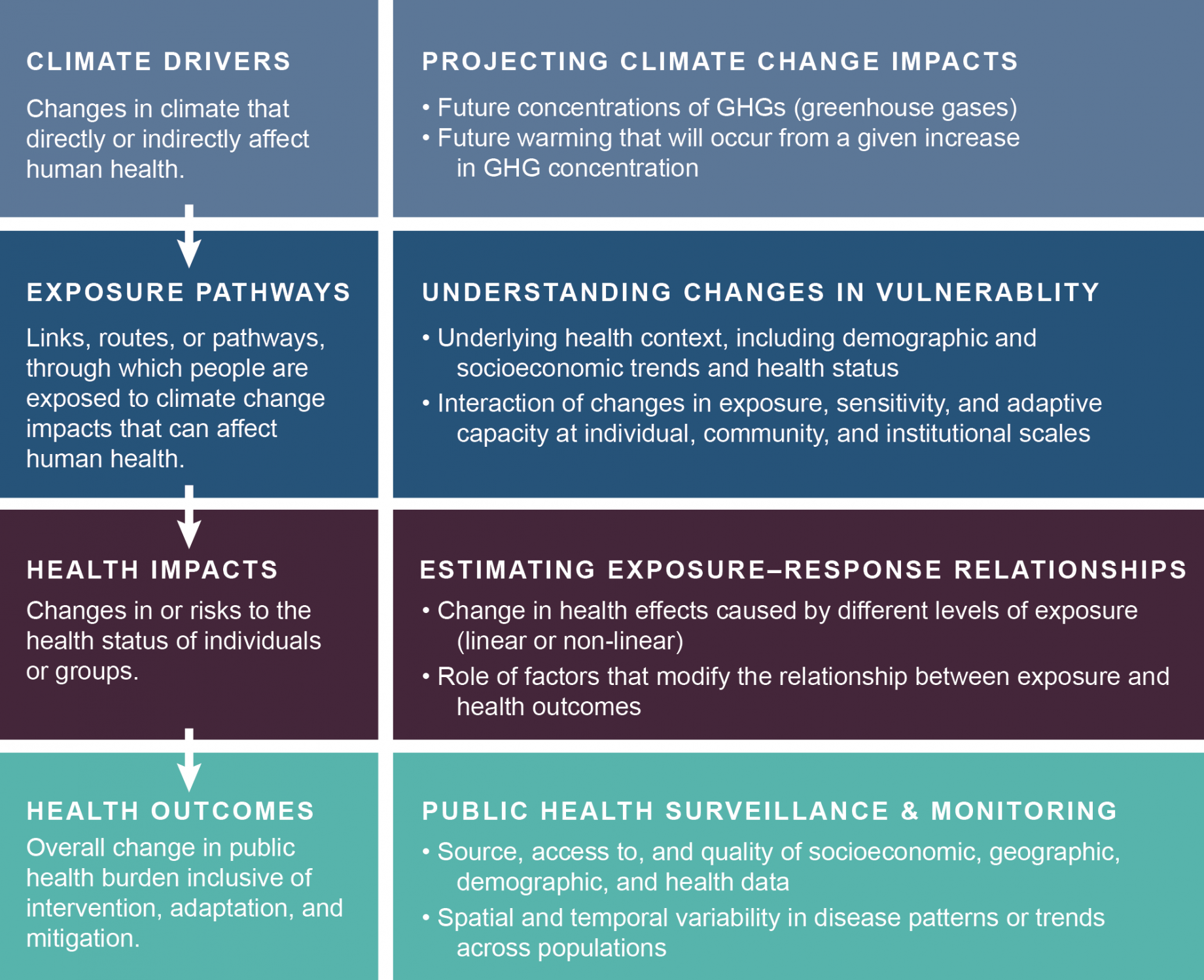
Examples of sources of
in projecting impacts of
on human
. The left column illustrates the
pathway through which climate alter can affect human wellness. The right column lists examples of cardinal sources of uncertainty surrounding effects of climate change at each stage along the exposure pathway.
Two of the key uncertainties in projecting future global temperatures are 1) uncertainty about hereafter concentrations of
Uncertainty in current and future estimates of health or
The factors related to uncertainty in exposure–response functions are similar to those for the projections of health or socioeconomic status. Estimates are more uncertain for smaller subpopulations, less-prevalent wellness conditions, and smaller geographic areas. Because these estimates are based on observations of existent populations, their validity when applied to populations in the future is more uncertain the further into the future the application occurs. Doubtfulness in the estimates of the exposure–outcome human relationship also comes from factors related to the scientific quality of relevant studies, including appropriateness of methods, source of data, and size of written report populations. Practiced judgment is used to evaluate the validity of an individual written report equally well as the collected grouping of relevant studies in assessing dubiousness in estimates of exposure–outcome relationships.
Approach to Reporting Uncertainty in Central Findings
Despite the sources of uncertainty described above, the current state of the science allows an examination of the likely direction of and trends in the health impacts of climatic change. Over the past ten years, the models used for climate and health assessments have go more useful and more than accurate (for example, Melillo et al. 2014).6 , 53 , 54 This cess builds on that improved capability. A more detailed discussion of the approaches to addressing dubiousness from the various sources can be constitute in the Guide to the Report and Appendix one: Technical Support Document.
Ii kinds of language are used when describing the uncertainty associated with specific statements in this report: confidence linguistic communication and likelihood linguistic communication (run across below). Confidence in the validity of a finding is expressed qualitatively and is based on the type, corporeality, quality, strength, and consistency of prove and the degree of expert agreement on the finding. Likelihood, or the projected probability of an impact occurring, is based on quantitative estimates or measures of uncertainty expressed probabilistically (in other words, based on statistical analysis of observations or model results, or on practiced judgment). Whether a Primal Finding has a confidence level associated with it or, where findings tin be quantified, both a confidence and likelihood level associated with information technology, involves the skilful assessment and consensus of the chapter writer teams.
Likelihood and Confidence Level
Likelihood
| Very Likely ≥9 in 10 | Likely ≥2 in 3 | Equally Likely as Not ≈ ane in 2 | Unlikely ≤ 1 in 3 | Very Unlikely ≤1 in 10 |
Confidence Level
Very High Strong evidence (established theory, multiple sources, consequent results, well documented and accepted methods, etc.), high consensus
High Moderate testify (several sources, some consistency, methods vary and/or documentation limited, etc.), medium consensus
Medium Suggestive bear witness (a few sources, limited consistency, models incomplete, methods emerging, etc.), competing schools of idea
Low Inconclusive bear witness (limited sources, extrapolations, inconsistent findings, poor documentation and/or methods not tested, etc.), disagreement or lack of opinions among experts
References
Source: https://health2016.globalchange.gov/climate-change-and-human-health
0 Response to "Explain How Climate and Temperature Can Affect the Behavior of Individuals."
Post a Comment